My name
c/o Froedtert Hospital Inpatient BMT
CFAC 9th Floor, Room 6
9200 W. Wisconsin Ave.
Milwaukee, WI 53226

Day -5 has been another long one. The first day in the hospital isn't exactly restful under the best circumstances, but as I'd posted yesterday, there are a LOT of interruptions now. Starting at midnight I had a bunch of blood drawn (baseline tests for blood infections from the central line x2 plus routine labs). 4:00 am was vitals. 5:00 am was pre-meds. 6:00 am started the busulfan, so I had to quick order and eat breakfast and then began cryotherapy (sucking on ice) from 7:30-9:30. They ran a bunch more labs after the first busulfan which lasted periodically until 2:00. And I was wrong--although I got the fludarabine at 5:00 yesterday, I'll get it at 2:00 from now on.
 |
| two cups of ice chips plus two orange popsicles to prevent mouth sores |
The dietician came and shared all sorts of useful information. There's a "secret menu" that allows me to order some items from the other restaurants at Froedtert. For lunch I had a French Dip sandwich, which was pretty good. I got a supplementary menu that lists all the high protein items on the regular menu, so I can make better choices when I get to that point. She explained that transplant recipients have a very high metabolism, so even if I eat "normally," I'll keep dropping weight. I will also, with all the GI stuff coming up, get to a point where I'll need protein shakes/smoothies. But they have a bunch of additional choices beyond a can of Ensure. She also suggested having the nurses put any smoothie or shake in the freezer for a bit because they're better when very cold. Ugh... I am just dreading that part of the stay. I have to remember that it will be temporary and that my body will need protein to recover, however I'm able to get it.
PT came by after lunch when I was trying to nap. I opened my eyes, focused on her name tag, and practically yelled, "PHYSICAL THERAPY! I'VE BEEN WAITING FOR YOU!" She told me that PT is usually not greeted that way by inpatients. :) I did my assessments for baseline and got a tour of the "gym," which has a bike-like machine, called a NuStep. It doesn't circle the pedals like a bike--just goes back and forth to strengthen other muscles. It also has arms that move back and forth--kind of like a recumbent elliptical! After I rode that for awhile, I asked if by chance there were any stationary bikes elsewhere in the hospital that I could use in my room. My room has plenty of space, and if I stay in it, I don't have to wear a mask. She said that they had one for patients in isolation but since no one is currently in isolation, I could keep it in my room. So now I have my own bike for the time being!

She also left me some resistance bands and exercises to do. In a non-COVID world there would be group exercise classes, including yoga. Now everything is individual.
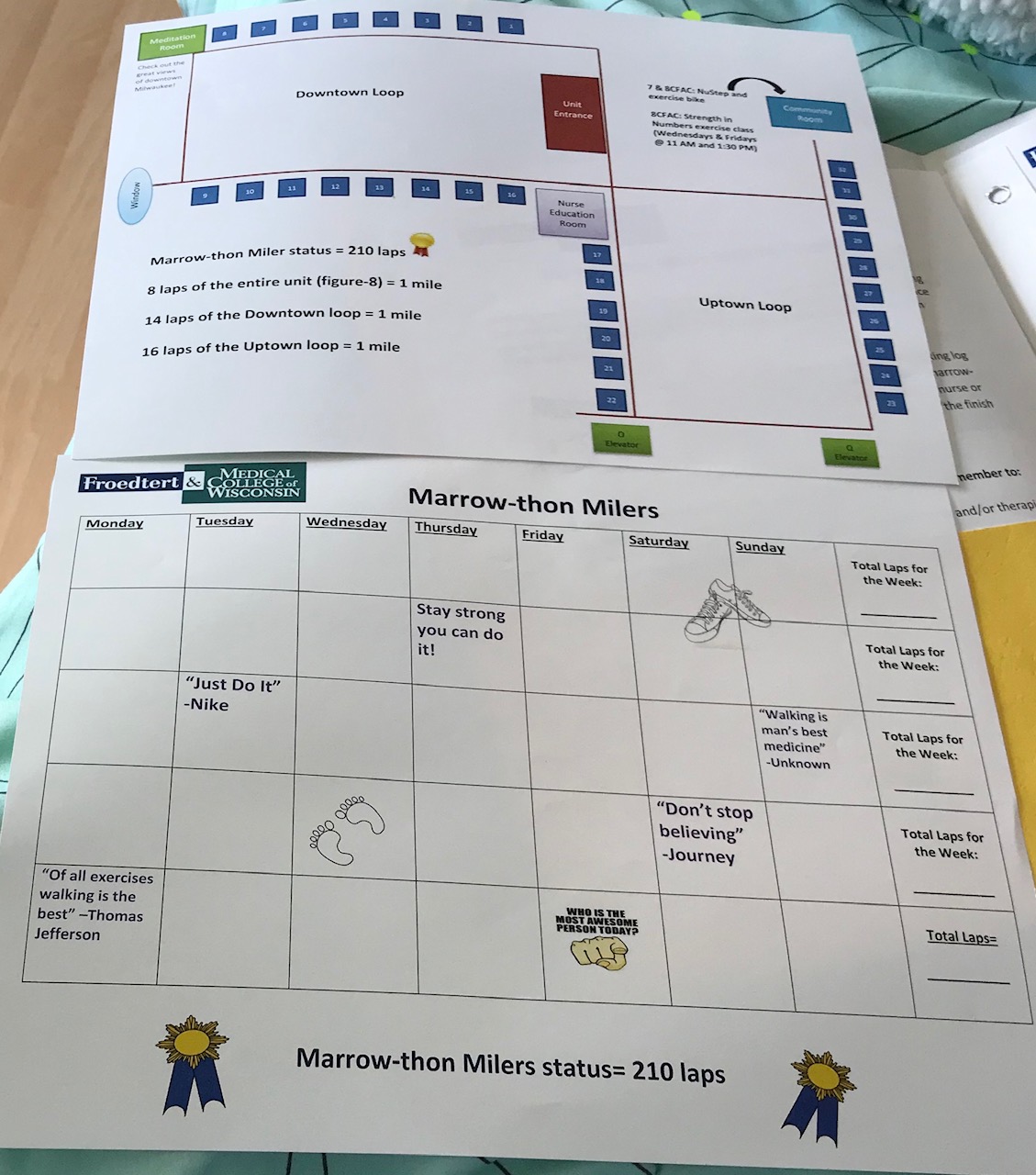
I've continued walking laps. I got the details on the Marrow-thon, which is met if you walk a total of 210 laps. One of the nurses was teasing me for walking so much right away, and she said that she had one patient who completed FOUR marrow-thons during his stay. Guess I have a goal to beat... LOL
Every staff member has been wonderful here. I would obviously rather have my family and friends around during this, but it's so nice to have good people to interact with. Pretty sure I'm already known as the chatty one.
Thank you all for your wonderful messages and bike rides (and walks and runs and strength workouts) for me and for sharing them on Facebook. (If you aren't in the group yet, and are interested, my friend Jill set up a Facebook page called Ride4lori. She posted a big scavenger hunt of things to find on your own bike rides, runs or walks, and to post in the group for me while I'm in the hospital and can't get outdoors. Feel free to join!
And now I'm off to walk again and then shower and try to get to bed early. Hugs to you all.




